
Measles Facts
For information about Dr Mendelsohn’s widely acclaimed and highly recommended book click HERE
MEASLES – by Dr Robert S Mendelsohn MD
Do You Want to Remain Informed about the Latest Vaccine News?
Measles, also called rubeola or English measles, is a contagious viral disease. At the onset the victim feels tired, has a slight fever and pain in the head and back. The eyes redden and may be sensitive to light. The fever rises until about the third or fourth day, when it reaches 103-104 degrees (this is the equivalent of about 40°C. Dr Mendelsohn’s wonderful book featured at the top of this page has an entire chapter about the role and the importance of fever in dealing with an infection and about the harm which is caused by fever-lowering drugs such as Tylenol/Paracetamol etc.- Erwin). Sometimes small white spots can be seen inside the mouth, and a rash of small pink spots appears below the hair line and behind the ears. This rash spreads downward to cover the body in about 36 hours. The pink spots may run together but fade away in about three or four days.

Measles is contagious for seven or eight days, beginning three or four days be-fore the rash appears. Consequently, if one of your children contracts the disease, the others probably will have been exposed to it before you know the first I child is sick.
No treatment is required for measles other than bed rest, fluids to combat possible dehydration from fever, and calamine lotion or cornstarch baths to relieve the itching. If the child suffers from photophobia, the blinds in his bedroom should be lowered to darken the room. However, contrary to the popular myth, there is no danger of permanent blindness from this disease.
A vaccine to prevent measles is an-other element of the MMR inoculation given in early childhood. Doctors maintain that the inoculation is necessary to prevent measles encephalitis, which they say occurs about once in 1,000 cases. After decades of experience with measles, I question this statistic, and so do many other paediatricians. The incidence of 1/1,000 may be accurate for children who live in conditions of poverty and malnutrition, but in the middle-and upper-income brackets, if one excludes simple sleepiness from the measles itself, the incidence of true encephalitis is probably more like 1/10,000 or 1/100,000.
After frightening you with the unlikely possibility of measles encephalitis, your doctor can rarely be counted on to tell you of the dangers associated with the vaccine he uses to prevent it. The measles vaccine is associated with encephalopathy and with a series of other complications such as SSPE (subacute sclerosing panencephalitis), which causes hardening of the brain and is invariably fatal.
Other neurologic and sometimes fatal conditions associated with the measles vaccine include ataxia (inability to coordinate muscle movements), mental retardation, aseptic meningitis, seizure disorders, and hemiparesis (paralysis affecting one side of the body). Secondary complications associated with the vaccine may be even more frightening. They include encephalitis, juvenile-onset diabetes, Reye’s syndrome, and multiple sclerosis.
I would consider the risks associated with measles vaccination unacceptable even if there were convincing evidence that the vaccine works. There isn’t. While there has been a decline in the incidence of the disease, it began long before the vaccine was introduced. In 1958 there were about 800,000 cases of measles in the United States, but by 1962-the year before a vaccine appeared-the number of cases had dropped by 300,000. During the next four years, while children were being vaccinated with an ineffective and now abandoned “killed virus” vaccine, the number of cases dropped another 300,000. In 1900 there were 13.3 measles deaths per 100,000 population. By 1955, before the first measles shot, the death rate had declined 97.7 percent to only 0.03 deaths per 100,000.
 Graph SOURCE
Graph SOURCE
Those numbers alone are dramatic evidence that measles was disappearing before the vaccine was introduced. If you fail to find them sufficiently convincing, consider this: in a 1978 survey of thirty states, more than half of the children who contracted measles had been adequately vaccinated. Moreover, according to the World Health Organization, the chances are about fifteen times greater that measles will be contracted by those vaccinated for them than by those who are not.
“Why,” you may ask, “in the face of these facts, do doctors continue to give the shots?” The answer may lie in an episode that occurred in California fourteen years after the measles vaccine was introduced. Los Angeles suffered a severe measles epidemic during that year, and parents were urged to vaccinate all children six months of age and older-despite a Public Health Service warning that vaccinating children below the age of one year was useless and potentially harmful.
Although Los Angeles doctors responded by routinely shooting measles vaccine into very kid they could get their hands on, several local physicians familiar with the suspected problems of immunologic failure and “slow virus” dangers chose not to vaccinate their own infant children. Unlike their patients, who weren’t told, they realized that “slow viruses” found in all live vaccines, and particularly in the measles vaccine, can hide in human tissue for years. They may emerge later in the form of encephalitis, multiple sclerosis, and as potential seeds for the development and growth of cancer.
One Los Angeles physician who refused to vaccinate his own seven-month-old baby said: “I’m worried about what happens when the vaccine virus may not only offer little protection against measles but may also stay around in the body, working in a way we don’t know much about.” His concern about the possibility of these consequences for his own child, however, did not cause him to stop vaccinating his infant patients. He rationalized this contradictory behaviour with the comment that “As a parent, I have the luxury of making a choice for my child. As a physician… legally and professionally I have to accept the recommendations of the profession, which is what we also had to do with the whole Swine Flu business.”
Perhaps it is time that lay parents and their children are granted the same luxury that doctors and their children enjoy.
————————————————

MEASLES – by Hilary Butler
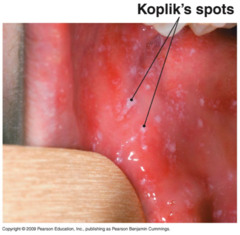
In the early stages of the cough, runny nose and fever, a child with Measles will get KOPLIK SPOTS which look like bluey-white grains of salt. These are best seen on the inside of the cheek near the second upper molar, but may also be on the gums anywhere in the mouth. They last for a few days, and are SPECIFIC for measles only. (Medicine International, 1984, pg 20, Viral Diseases in Man, 83rd Edition, pg 412.) Why do you need a painful blood-test with such a specific sign easily available?
You should NOT take your child to the doctor at this initial stage if your child has KOPLIK SPOTS as this is the MOST infective stage. If necessary, ring the surgery, but there is nothing your medically responsible doctor should, or could prescribe for your child at this stage. Studies have shown that children taken to doctor’s surgeries, health care facilities and hospitals at this highly infectious stage increase the spread of measles, and put at risk the very people for whom measles is so dangerous – sick or immunocompromised adults, babies and other children. (Infect Dis Child, Dec 95; Ped Infct Dis, Jan 93; Maryland Med J, Oct 91.)
There is a “cure” for measles. It is called Vitamin A…Cod-liver oil. As early as 1932, doctors used cod-liver oil to reduce hospital mortality by 57%, but then antibiotics became the treatment of fashion, and Vitamin A was thrown out until the mid-80’s.

Recent published studies have found that 72% of hospitalised measles cases in America are Vitamin A deficient, and the worse the deficiency, the worse the complications and higher the death rate. (Pediatric Nursing, Sept/Oct 1996.) Yet doctors and hospitals in New Zealand do not use Vitamin A.
(Light-sensitive or sore eyes in children with measles are a sign that the body has used up its stores of vitamin A to deal with the measles infection and that vitamin A supplementation is indicated – Erwin)
FACT: 1991 Six deaths, 4 younger than 12 month , unvaccinated, died of pneumonia/encephalitis. 2 vaccinated children, deaths encephalitis.
FACT: THESE CHILDREN WERE NOT TREATED WITH VITAMIN A (Q: IF THEY HAD BEEN, WOULD THEY HAVE DIED?)
The Health Department says that keeping unvaccinated healthy children away from vaccinated children will protect vaccinated children. They tell us that vaccines protect children, so aren’t they already vaccine “protected”? The answer is NO. In 1991 over 60% of cases were in “vaccinated” children.
Question: Didn’t children used to get measles regularly? Health Department answer: “Yes, because there was no widespread immunisation… Deaths and hospitalisations from measles were not recorded.”
FACT. Vaccinated children still get measles. Deaths and hospitalisations have been recorded for 120 years. The measles death decline graph provided shows that the measles vaccine had nothing to do with the decline in deaths, and has not affected the number of children hospitalised during epidemic years since its introduction. (Appendices to Parliamentary Journals, Official Year Book, Health Department publications such has “Health Trends” and Immunisation Handbook. Also, graphs provided to Herald and Metro in the past)
PARENTS HAVE A RIGHT TO KNOW THAT:
*** A similar campaign vaccinating 7.1 million schoolchildren in England has resulted in a legal firm called Dawbarns (dawbarns @paston.co.uk) taking legal action against the British Health Department on behalf of the following cases:
Autism (202),
Crohn’s disease and other serious chronic stomach problems (110)
Epilepsy (97)
Hearing and vision problems (40)
Arthritis (42)
Chronic Fatigue Syndrome (24)
Diabetes (9)
Guillain-Barre syndrome (9)
Chronic Thrombocytopenia (5)
Subacute Sclerosing Panencephalitis SSPE {3)
Wegener’s Granulomatosis (2)
Multiple Sclerosis (1)
Death (14)
SOURCE: Dawbarns fact sheet
*** The childrens’ doctors and specialists have come out in the media in support of the children
*** The New Zealand, and British Health Departments deny the existence of these cases. (NZ H Dept media release, and BMJ article) and maintain that OPERATION SAFEGUARD eliminated measles from UK. In October 1996, UK started another MMR booster campaign.
**** Deaths from Measles were virtually wiped out in every developed country before the vaccine was even used – see disease decline graphs HERE
*** Using the Health Department statistics on vaccinating 540,000 children, would result in:
Up to 81,000 cases of rash and fever.
Up to 5,400 cases of parotid (mumps) swelling
Up to 216 cases of febrile seizures
Up to 18 cases of thrombocytopenia (red-blood cell destruction)
Up to cases of chronic thrombocytopenia.
Up to 5 cases of Aseptic Meningitis.
Up to 1 case of Central Nervous system damage.
Up to 15,420 cases of transient joint arthralgia some of these becoming chronic. (pg 95, H. Dept Handbook)
*** Germany did not routinely use the measles vaccine because their reporting system found 1 per 2,500 vaccinees had a neurological complication, and 1 per 17,500 vaccinees had abortive encephalopathy. (FDA Technical Report, 1980)
The Germans considered the risks too high in light of the fact that deaths and disease severity had decreased without any reference to a vaccine. THE SAME IS TRUE OF NEW ZEALAND, but parents are not told that. (The MMR vaccine is now however nevertheless part of the German childhood vaccination schedule HERE. In Switzerland, over 500 medical doctors formed an organisation to oppose the Swiss government’s introduction of the MMR vaccine into the Swiss vaccination schedule on the grounds that this three live viruses in one injection vaccine posed too great a risk for children. – Erwin).
*** That in the pre-vaccine era, mothers’ antibodies protected babies for around 15 months, measles was mainly an infection of 5 – 9-year-olds, and by 15 yrs, 99% had antibodies. By 1985, 14 % of 15-year-olds lacked antibody.( NZ Med J. 27 May, 1987) No-one knows what the level is now, but evidence from America shows that adult measles, which can be very serious, is now quite common.
*** that vaccinated mothers cannot give protective antibodies to their babies, so that young babies, for whom measles is serious are no longer protected. (Washington Post, Sun Nov 22, 1992, and others)
“** that in the 1991 USA measles outbreak, over half of those who died were vaccinated, and most deaths were in immunocompromised people. (Washington Post June 14, 1991, BMJ, 11 May, 1991)
*** that New Zealand doctors and hospitals do not prescribe or use Vitamin A for measles, and as a result, many cases are far more serious than they should be.
“** that in Africa, children who have a natural measles infection have half the asthma, allergies and eczema compared with their vaccinated peers. (Lancet, June 29, 1996)
*** that if children with mild to moderate psoriasis get a natural dose of measles, the psoriasis is often cured. (3 med studies)
*** that babies vaccinated who have maternal antibodies, or people who have measles suppressed with gammaglobulin go on to have a higher rate of immunoreactive diseases, sebaceous skin diseases, degenerative cartilage and bone disease and certain tumours. (Lancet, 5 Jan 1985)
Q: If you revaccinate children who already have antibodies what will happen to them in later life?
*** that you have the right to take home the PRODUCT INSERT, and read it carefully before you make any decision”.
*** in New Zealand parents have freedom of choice concerning vaccination.
IF YOU CHOOSE TO VACCINATE YOUR CHILD WITH MMR and anything happens which you know is not normal for your child, go to your doctor, or hospital immediately. In New Zealand, fill out an H 1574 form and send it to CARM, make sure that the medical records are correct, sign them yourself, and get copies. In the event of permanent damage, without these documents you will be unable to obtain ACC coverage (compensation via the NZ Accident Compensation Corporation – Erwin) or financial assistance of any sort.(In other countries parents likewise need to ensure that the doctor reports the reaction to the appropriate government agency and if he doesn’t, to report it themselves – Erwin).
Excerpted and slightly edited from ‘Measles: The Real Facts’ by Hilary Butler HERE
————————————————

Ineffectiveness of Measles Vaccination and Unintended Consequences. ~ by Dr Viera Scheibner (PhD)
– January 18, 2013
Measles vaccine introduction
Measles vaccination in the US and many other countries started in the early 1960s, at the time when measles was naturally abating and was heading for the 18 year low. That’s why the vaccine seemingly lowered the incidence; however, this was only coincidental with the natural dynamics of measles.
As one of many examples involving all infectious diseases of childhood against which vaccines have been developed, ever since any measles vaccines have been introduced and used in mass proportions, reports of outbreaks and epidemics of measles in even 100% vaccinated populations started filling pages in medical journals.
Reports of serious reactions including deaths also appeared with increasing frequency. They are the subject of a separate essay.
Atypical measles – a new phenomenon only in the vaccinated
It is less well known to the general public that vaccinated children started developing an especially vicious form of measles, due to the altered host immune response caused by the deleterious effect of the measles vaccines. It resisted all orthodox treatment and carried a high mortality rate.
It has become known as atypical measles. (AMS)
Rauh and Schmidt (1965) described nine cases of AMS which occurred in 1963 during a measles epidemic in Cincinnati. The authors followed 386 children who had received three doses of killed measles virus vaccine in 1961. Of these 386 children, 125 had been exposed to measles and 54 developed it [i.e. measles].
The new, atypical measles, occurring in the vaccinated was characterised by high fever, unusual rash and pneumonia, often with history of vaccination with killed measles vaccine.
Rauh and Schmidt (1965) concluded that, “It is obvious that three injections of killed vaccine had not protected a large percentage of children against measles when exposed within a period of two-and-a-half years after immunization”.
Fulginiti (1967) also described the occurrence of atypical measles in ten children who had received inactivated (killed) measles virus vaccine five to six years previously.
Nichols (1979) wrote that atypical measles is generally thought to be a hypersensitivity response to natural measles infection in individuals who have previously received killed measles vaccine, although several investigators have reported AMS-like illness in children who had been vaccinated only with live measles vaccine.
He wrote that during a measles epidemic in 1974-1975 in Northern California, a number of physicians reported laboratory-confirmed measles in patients who had signs and symptoms, compatible with AMS…”We developed case criteria on the basis of serology and rash distribution and morphology. In typical measles a maculopapular rash occurs first at the hairline, progresses caudally, is concentrated on the face and trunk, and is often accompanied by Koplik’s spots. In AMS the rash Is morphologically a mixture of maculopapular, petechial, vesicular, and urticarial components. It usually begins and is concentrated primarily on the extremities, progresses cephalad, and is not accompanied by Koplik’s spots. Cases were classified as AMS if patients had 1) a rash with the distribution and morphology characteristic of AMS, and 2) a fourfold or greater rise in titer of complement-fixing measles antibody or a convalescent titer of 256”.
Continuing measles outbreaks signal increasing incidence comparable with the pre-vaccine era.
In the meantime, outbreaks of measles in vaccinated children have continued and intensified to this day. Contemporary observations of the ineffectiveness of vaccination indicate to me that the incidence of measles has increased and has not continued decreasing as it did for some 100 years before any type of measles vaccination was introduced.
Conrad et al. (1971) published about the dynamics of measles in the US in the last four years and conceded that measles was on the increase and that “eradication, if possible, now seems far in the future”.
Barratta et al. (1970) investigated an outbreak in Florida from December 1968 to February 1969 and found little difference in the incidence of measles in vaccinated and unvaccinated children.
Right through the 1980s, measles outbreaks in fully vaccinated children have continued all over the US and all other countries with high vaccination rates all over the world.
Robertson et al. (1992) wrote that in 1985 and 1986. 152 measles outbreaks in US school-age children occurred among persons who had previously received measles vaccine. “Every 2-3 years, there is an upsurge of measles irrespective of vaccination compliance”.
To cap it all: the largely unvaccinated Amish (they claim religious exemption) had not reported a single case of measles between 1970 and December 1987, for 18 years (Sutter et al. 1991). It is quite likely that a similar situation would have applied to outside communities without any vaccination and that measles vaccination had actually kept measles alive and kicking. According to Hedrich (1933), there is a variety of dynamics of measles occurrence, from 2-3 years to up to 18 years, as later also witnessed by the unvaccinated Amish.
MMWR (2009) reported that the US Centers for Disease Control and Prevention (CDC) had reminded physicians about the importance of immunization against measles in response to outbreaks of the disease in the US. 64 cases of measles were noted between January 1 and April 15 2008.
“Measles outbreaks in Africa threatens gains” reported by Voice of America, July 9, 2010. “…nearly 90,000 cases of measles have occurred in Sub-Saharan Africa since June 2009, including about 1,400 deaths”.
Shi et al. (2011) reported on measles incidence rate and a phylogenetic study of contemporary genotype H1 measles strains in China, calling for a new vaccine, since the incidence of measles in China has increased over the last decade.
A widespread outbreak of measles was reported across Europe during European Immunization Week (April 25, 2011). Some 6,500 cases of measles were reported in 30 countries according to WHO’s press release.
MMWR Wkly Rep 2012; 61: 253-257 reported a quadruple increase in the incidence of measles in 2011. Even though the absolute numbers appear small, the actual numbers were no doubt in my mind much higher. The outbreaks were blamed on imported measles cases. [Isn’t the vaccine supposed to protect the vaccinated when in contact with someone with measles?]
Instead of discontinuing vaccination with obviously ineffective and dangerous vaccines, re-vaccination, meaning further doses of the ineffective measles vaccines and the development of new vaccines are being recommended.
Linnemann et al. (1973) concluded that measles vaccines were not provoking a proper immunological response in vaccinated children.
Black et al. (1984) summarized data on the ineffectiveness of re-vaccination published by several authors, who demonstrated that “antibody titer in re-immunised children may fall after several months to very low levels, and that children vaccinated twice may still experience clinically recognizable measles, although in a much milder form ”. They concluded that, “this state in which a child is immunologically sensitized, but not immune to infection, we shall call inadequate immunity.”
Unfounded optimism for measles eradication in the US by 1 October 1982
Despite the obvious lack of success with measles vaccination, in October 1978, the Secretary of the Department of Health, Joseph A Califano Jr. announced, “We are launching an effort that seeks to free the United States from measles by 1 October 1982″.
Predictably, this unrealistic plan fell flatly on its face: after 1982 the US was hit repeatedly by major and even more sustained epidemics of measles, mostly in fully vaccinated populations. First, the blame was laid upon the “ineffective, formalin-inactivated (‘killed’) measles vaccine, administered to hundreds of thousands of children from 1963 to 1967″. However, outbreaks and epidemics of measles continued occurring even when this first vaccine was replaced with two doses of ‘live’ measles virus vaccines and the age of administration was changed.
These warnings have not been heeded. As the Swiss doctors wrote (Albonico et al. 1990), “we have lost the common sense and wisdom that used to prevail in the approach to childhood diseases. Too often, instead of reinforcing the organism’s defences, fever and symptoms are relentlessly suppressed. This is not always without consequences”.
Destruction of transplacentally-transmitted immunity by vaccination
Many researchers warned straight after the introduction of measles vaccine in the US that the generations of children born to mothers who were vaccinated in childhood will be born with poor or no transplacentally-transmitted immunity and will contract measles and other diseases too early in life.
Lennon and Black (1986) demonstrated that “haemaglutinin-inhibiting and neutralizing antibody titers are lower in women young enough to have been immunized by vaccination than older women”. The same applied to whooping cough. It explains why so many babies before vaccination age develop these diseases, and most particularly the much publicised whooping cough.
Deranged cholesterol due to measles vaccination
Soon after measles mass vaccination started, concerns about increased cholesterol levels and deranged ratio of high-density to low-density lipids in young children started filling pages in the medical press.
Vikari et al. (1979. Effect of measles and measles vaccine on serum cholesterol. Lancet; February 10: 326) quoted Drs Matthews and Feery (1978) who “…reported that immunisation with influenza vaccine seemed to be followed by an increase in serum-total-cholesterol and by a decrease in HDL cholesterol. They suggested that immunisation with viral antigens or natural virus infection might contribute to variation in lipid levels”.
And, “We have measured serum-total-cholesterol in 97 children (average age 2 years) before and 6 weeks after measles vaccination (Rimevax, R.I.T. Belgium) and in serial serum samples of 27 measles patients (average age 4 years). Children were fed ad libitum. Antibody titres were assayed by haemagglutination inhibition and serum-cholesterol was measured with the method of Leppilnen. Samples from the same child were measured in the same series”.
“Five children showed exceptionally high relative increase (more than or equal to 40%) of serum-cholesterol after vaccination, although the absolute values remained within normal limits. No correlations were observed between the initial cholesterol values or changes in cholesterol values and measles antibody responses. After 8 and 10 months the relative increase of serum-cholesterol was still recorded in two children. After natural measles infection the mean serum-cholesterol was low in the specimens collected 1-7 days after the onset of symptoms…”
Vikari et al. (1979) then concluded, “Our data show that natural measles decreases serum-cholesterol values in the acute phase of the disease. This accords with the observations of Lees et al., who showed that experimental infection with sandfly virus infection decreased serum-cholesterol values for at least 10 days. Whether the same kind of decrease of cholesterol level occurs also after measles vaccination and, possibly, after other virus vaccinations needs to be clarified. Our observations support the view presented by Matthews and Feery (1978) that natural virus infection or immunisation with viral antigens induces changes in serum-lipid levels in man”.
Bell et al. (2012) wrote, “In a large population-based sample of Australian school children we found a higher frequency of abnormal lipid profiles when compared to American data. In addition, many children have levels outside reported healthy norms for Australian children. Research tracking lipid profiles of Australian children to adulthood is needed to understand the association of these levels with future cardiovascular risk”.
In her 72-page doctoral thesis, Louise Strandberg (2009) looked at length and exhaustively into interactions between nutrition, obesity, and the immune system.
Importantly, she writes, “In the 1950’s, it was first recognised that dietary fat could contribute to cardiovascular diseases in the Western World. However, the Greenland Eskimos were known to eat large amounts of fat but still had a very low incidence of cardiovascular disease. In the 1970ies, Bang and Dyerberg found that the Eskimos had low levels of cholesterol and lipoproteins, except for the high-density lipoproteins that is [sic] now known as “the good cholesterol…quality of dietary fat rather than quantity is important for development of cardiovascular disease”.
That would have represented the generation of non-vaccinated Eskimos.
Based on medical research, a logical conclusion is that an important primary cause of the observed abnormal cholesterol and triglyceride levels in children may be an invasive medical intervention in the form of vaccination.
Relevant reading
Rauh LW, and Schmidt R. 1965. Measles immunization with killed virus vaccine. Am J Dis Child; 109: 232-237.
Fulginiti VA, Eller JJ, Downie AW, and Kempe CH. 1967. Altered reactivity to measles virus. Atypical measles in children previously inoculated with killed-virus vaccines. JAMA; 202 (12): 1075-1080.
Scott TF, and Bonanno DE 1967. Reactions to live-measles-virus vaccine in children previously inoculated with killed-virus vaccine. NEJM; 277 (5): 248-251.
Barratta RO, Ginter MC, Price MA, Walker JW, Skinner RG. et al. 1970. Measles (Rubeola) in previously immunized children. Pediatrics; 46 (3): 397-402.
Conrad JL, Wallace R, and Witte JJ. 1971. The epidemiologic rationale for the failure to eradicate measles in the United States. Am J Publ Health; 61 (11):2304-2310.
Linnemann CC, Hegg ME Rotte TC et al. 1973. Measles MgE response during re-infection of previously vaccinated children. J Pediatrics; 82: 798-801.
Gustafson TL, Lievens AW, Brunell PA, Moellenberg RG, Christopher BS et al. 1987. Measles outbreak in a fully immunized secondary-school population. NEJM; 316 (13): 771-774.
Black EI, Berman LL, Reichelt CA, de Pinheiro P et al. 1984. Inadequate immunity to measles in children vaccinated at an early age: effect of revacination. BULL WHO; 62 (92): 315-319.
Robertson SE, Markowitz LE, Dini EF, and Orenstein WA. 1992. A million dollar measles outbreak: epidemiology, risk factors, and selective revaccination strategy. Publ Health Reports; 197 (1): 24-31.
Sutter RW, Markowitz LE, Bennetch JM, Morris W, Zell ER and Preblud WSR. 1991. Measles among the Amish: a comparative study of measles severity in primary and secondary cases in households. J Infect Dis; 163: 12-16.
Hedrich AW. 1933. Monthly estimates of the child population “susceptible” to measles, 1900-1931, Baltimore, MD. Am J Hygiene: 613- 635.
Lennon and Black 1986. Maternally derived measles immunity in era of vaccine-protected mothers. J Pediatr; 108 (1): 671-676.
Matthews and Feery 1978, Lancet ii: 1212-1213.
Bell et al. (2012. Lipids in Australian children: cause for concern? 2005-2007 Busselton Health Study. J Paediatr & Child Health; Oct 2012: 863-953).
SOURCE
————————————————–
Benefits of Contracting Measles ~ by Dr Viera Scheibner (PhD)
January 29, 2013
Well-managed natural infectious diseases are beneficial for children.
When infectious diseases of childhood are not mismanaged by the administration of antibiotics, or by suppressing fever, the diseases prime and mature the immune system and also represent developmental milestones.
Having measles not only results in life-long specific immunity to measles, but also in life-long non-specific immunity to degenerative diseases of bone and cartilage, sebaceous skin diseases, immunoreactive diseases and certain tumours as demonstrated by Ronne (1985).
Having mumps protects against ovarian cancer (West 1969).
This is the area that should be researched and the results heeded instead of trying the impossible: to eradicate infectious diseases.
Approaching childhood diseases with common sense and wisdom.
The already quoted large group of Swiss doctors that formed a working committee questioning the Swiss’ Health Department’s policy of mass vaccination with the MMR (measles, mumps and rubella) vaccine, wrote that up to 1969, at the Basel University Paediatric Clinic, artificial infection with measles was used to treat successfully the nephrotic syndrome (Albonico et al. 1990).
Asthma and allergies prevented by natural measles disease.
As shown by Shaheen et al. (1996), even in a developing country having measles is beneficial: it prevents atopy: “After adjustment for breastfeeding and other variables, measles infection was associated with a large reduction in the risk of skin-prick test positivity to household dustmite . . . 17 (12.8%) of 133 participants who had had measles infection were atopic compared with 33 (25.6%) of 129 of those who had been vaccinated and not had had measles”.
Alm et al. (1999) wrote that increased prevalence of atopic disorders in children may be associated with changes in types of childhood infections, vaccination programmes, and intestinal microflora.
They found that at the Steiner schools in Sweden, “52% of the children had had antibiotics in the past, compared with 90% in the control schools…18% and 93% of children respectively, had had combined immunisation against measles, mumps, and rubella, and 61% of the children at the Steiner schools had had measles”.
“Fermented vegetables, containing live lactobacilli, consumed by 63% of the children at Steiner schools, were compared with 4.5% at the control schools….Skin-prick tests and blood tests showed that the children from Steiner schools had lower prevalence of atopy than controls”.
Engineered measles virus used in anti-cancer therapy.
Carmona Mota (1973) described a remission of infantile Hodgkin’s disease after natural measles. They wrote, “A 23-months-old Caucasian male was seen for the first time in April 1970 with a large mass in the neck due to hypertrophy of the left cervical lymph nodes. Before radiotherapy could be started the child developed measles. Much to our surprise the large cervical mass vanished without further therapy.”
Many others started researching and writing about the oncolytic (cancer-destroying) effect of measles virus.
Msaouel et al. (2009) conducted clinical testing of engineered oncolytic measles virus strains in the treatment of cancer. Even though the virus they used was a vaccine-type virus, the research was done in vitro with a virus directly injected into the tumour. They wrote, “It is of note that a number of viral strains, including certain derivatives of the attenuated live measles virus Edmonston (MV-Edm) vaccine strain, demonstrate a propensity to preferentially infect, propagate in, and destroy cancerous tissue.
The reason for using modified viruses was given as “concerns regarding the potential of wild-type-viruses to cause serious side effects, technical limitations in manufacturing viral lots of high purity for clinical use, as well as the overwhelming excitement and fervent support for the, at the time, newly emerging chemotherapy approaches that slowed down research on alternative strategies”.
One can reasonably speculate that there were also political reasons for using a vaccine measles virus (an engineered measles virus), and not the wild measles virus, because the next question to answer would be why not simply let children have the natural measles and thus achieve the long-term non-specific immunity to a number of cancers.
The dangers of medical interference in disease management.
It is disconcerting that as in the past, even today’s doctors still relentlessly suppress fever and administer antibiotics as part of the standard practice ignoring well-documented published research which demonstrated that suppressing fever at the same time as administering antibiotics (and other medications) encourages the growth and general viability of the pathogens and their ability to develop resistance to such medications and may lead to their increased virulence (Mackowiak (1981)).
I end with an important message from history, which unfortunately fell on deaf ears and which has not lost its relevance to modern medical practice.
In a letter to the Duchess Sophia, mother of the future George I of England, Princess Elizabeth Charlotte (Liselotte) von der Pfalz, Duchess of Orleans and widow of the younger brother of Louis XIV, wrote:
Our misfortune continues. The doctors have made the same mistake treating the little Dauphin as they did ministering to his mother, the Dauphiness. When the child was quite red from the rash and perspired profusely, they [the doctors] performed phlebotomy and administered strong emetics; the child died during these operations. Everybody knows that the doctors caused the death of the Dauphin, since his little brother who had the same sickness, was hidden away from the 9 physicians who were busy with his older brother, by the young maids, who have given him a little wine with biscuits. Yesterday, when the child had high fever, they wanted also to perform phlebotomy but his two governessess were firmly opposed to the idea and instead kept the child warm. This one also would have certainly died if the doctors had had their way.
I do not understand why they don’t learn by experience. Had they no heart, when they saw the Dauphiness die after phlebotomy and emetics, not to dispose of her child?
Koprowski (1962) summarised the still relevant historic message, ”Avoid physicians and thou will be cured.”
Summary
Despite their long history of failures and tragedies arising from their observed derailing effects on the immune system, outdated procedures for both disease prevention, i.e. vaccination, and disease management, i.e. treatment hostile to the body’s defences, such as antibiotics and anti-pyretics, remain standard practice to this day. The damage already done will continue to affect future generations for some time to come.
The unscientific standard procedures should be abandoned and the natural processes and the innate intelligence of the immune system respected. Medicine should adopt a common sense attitude to natural infectious diseases and their vital role in priming and maturing the immune system, for children’s long-term benefit.
Ronne T. 1985. Measles virus infection without rash in childhood is related to diseases in adult life. Lancet; 5 Jan: 1-5.
West RO. 1966. Epidemiologic studies of malignancies of the ovaries. Cancer; 1001-1007.
Albonico H et al 1990. Vaccination campaign against measles, mumps and rubella, A constraining project for a dubious future? Working group of doctors for selective MMR vaccination.18 pages, self-published.
Sheheen et al. 1996. Measles and atopy in Guinea-Bissau. Lancet; 347: 1792-1796.
Alm et al. (1999). Atopy in children of families with an anthroposophic lifestyle. Lancet; 353: 1485-1488.
Carmon Mota H. 1973. Infantile Hodgkins’disease: remission after measles. BMJ; 19May: 423.
Msaouel P, et al. 2009. Clinical testing of engineered oncolytic measles virus strains in the treatment of cancer: An overview. Curr Opin Mol Ther; February; 11(1): 43-53.
Mackowiak PA. 1981. Direct effects of hyperthermia on pathogenic microorganisms: teleologic implications with regard to fever. Rev Infect Dis; 3(3).
Koprowski H. 1962. The role of hyperergy in measles encephalitis. Am J Dis Child; 103:103-108.
RELATED:
– Vitamin A Treatment of Measles HERE

Baby Kash aged 14 Months, One Day After Vaccine Reaction to MMR
SOURCE/RELATED ARTICLE
– Child Health And Caring For A Sick Child – by Dr L Palevsky HERE
Why All The Measles Outbreaks?…
Melanie’s Marvellous Measles – by Stephanie Messenger
– Measles Outbreaks Centered in the Vaccinated: Studies Show Vaccine Is Ineffective HERE
– Measles outbreak in a fully immunized secondary-school population HERE
– The 2013 Measles Outbreak: A Failing Vaccine, Not A Failure To Vaccinate HERE
HIGHLY RECOMMENDED:
– This Mama Isn’t Scared of the Shmeasle Measles – by Megan – June 8, 2014

———————

– ZERO U.S. Measles Deaths in 10 Years, but Over 100 Measles Vaccine Deaths Reported
http://healthimpactnews.com/2015/zero-u-s-measles-deaths-in-10-years-but-over-100-measles-vaccine-deaths-reported/
– Measles outbreak in Europe: convenient lies
https://jonrappoport.wordpress.com/2017/07/25/measles-outbreak-in-europe-convenient-lies/
– Measles and Measles Vaccines: 14 Things To Consider
http://www.greenmedinfo.com/blog/measles-and-measles-vaccines-14-things-we-consider